

Post by Nadica (She/Her) on Oct 2, 2024 0:56:57 GMT
Study shows that COVID-19 causes cognitive decline among those without long COVID symptoms - Published Sept 24, 2024
By Bill Shaw
A new study in eClinicalMedicine has found that healthy volunteers infected with SARS-CoV-2 had measurably worse cognitive function for up to a year after infection when compared to uninfected controls. Significantly, infected controls did not report any symptoms related to these cognitive deficits, indicating that they were unaware of them. The net effect is that potentially billions of people worldwide with a history of COVID-19, but no symptoms of long COVID, could have persistent cognitive issues without knowing it.
The study’s lead author, Adam Hampshire, professor of cognitive and computational neuroscience at King's College London, said:
"It … is the first study to apply detailed and sensitive assessments of cognitive performance from pre to post infection under controlled conditions. In this respect, the study provides unique insights into the changes that occurred in cognitive and memory function amongst those who had mild COVID-19 illness early in the pandemic."
This news comes as pandemic mitigation measures have all but been abandoned by governments across the globe. Public health practice has been decimated to the point where even surveillance data on SARS-CoV-2 infections and resulting hospitalizations, deaths, and other outcomes are barely collected let alone published.
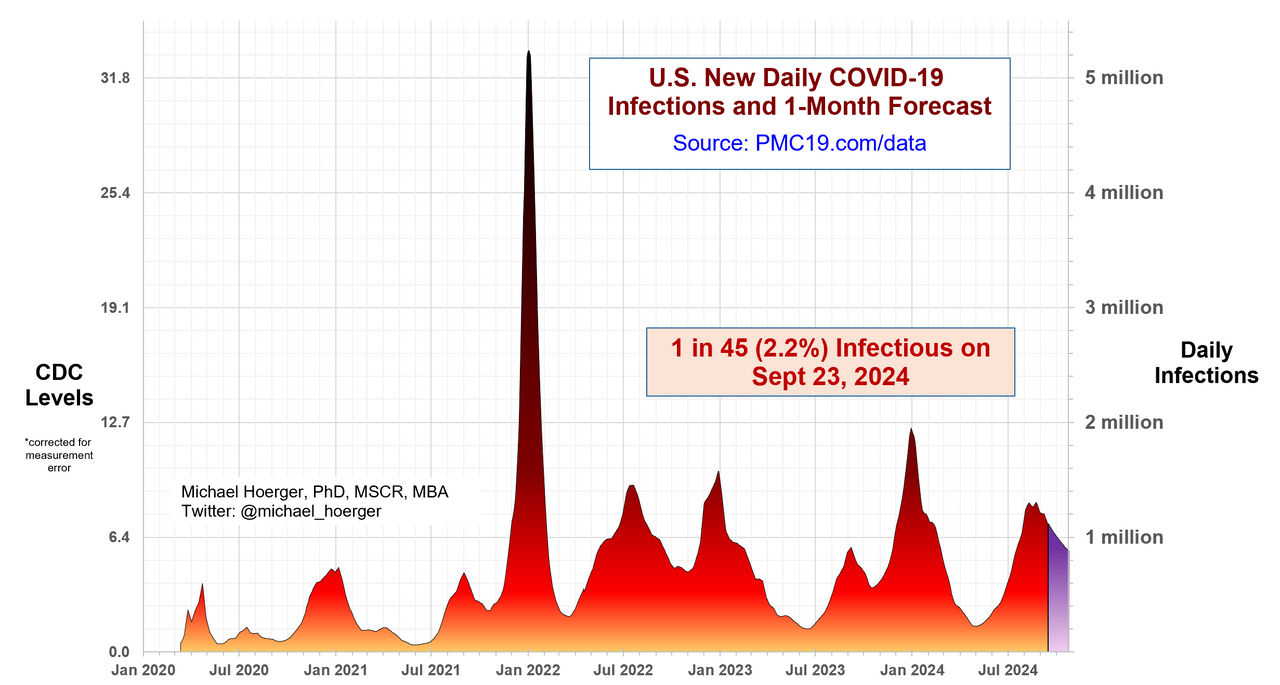
The data that are available indicate, per the most recent modeling from the Pandemic Mitigation Collaborative (PMC) on September 23, that since the beginning of August there have been over 1 million infections per day in the US alone. This level of transmission is expected to persist through the remainder of September and all of October. For the months of August through October, these levels of transmission are the highest of the entire pandemic
The study on cognitive deficits has been shared widely across social media, with scientists and anti-COVID advocates drawing out its dire implications.
Australian researcher and head of the Burnet Institute, Dr. Brendan Crabb, who has previously advocated for a global elimination strategy to stop the pandemic, wrote:
"Ethical issues aside, this is a powerful addition to an already strong dataset on Covid-driven brain damage affecting cognition & memory. Given new (re)infections remain common, this work… should influence a re-think on current prevention/treatment approaches."
The study enrolled 36 healthy volunteers. These individuals had no history of prior SARS-CoV-2 infection, no risk factors for severe COVID-19, and no history of SARS-CoV-2 vaccination. The researchers determined whether the volunteers were seronegative prior to inoculation, meaning that they had no detectable antibodies to SARS-CoV-2. If such antibodies were present, it would indicate past infection or vaccination.
These procedures resulted in a total of data from 34 volunteers being included for analysis. Two volunteers were excluded from analysis because they had seroconverted to positive for SARS-CoV-2 antibodies between the time of screening and inoculation. Notably, these two volunteers participated in all subsequent study activities, enabling a sensitivity analysis of the results that included them.
The researchers inoculated all 36 volunteers with SARS-CoV-2 virus in the nose and then quarantined them for at least 14 days. Volunteers only returned home once they had two consecutive daily nasal and throat swabs that were negative for virus. Thus, those volunteers who had an infection after inoculation spent the duration of their infection in quarantine. This quarantine was required by ethical study protocols, in order that the study itself not increase community transmission of the virus.
The researchers collected data on the volunteers daily during quarantine and at follow-up visits at 30, 90, 180, 270, and 360 days post-inoculation. The assessments included body temperature, viral loads from throat and nasal swabs, surveys on symptoms, and computer-based cognitive tests on 11 major cognitive tasks. The cognitive testing varied the particular exercise for each of the 11 tasks to avoid learning and memorization of solutions in subsequent sessions. Nevertheless, some tasks were more prone to learning so the researchers also studied the effect of infection on “learning” vs. “non-learning” tasks.
Of the 36 inoculated volunteers, 18 became infected and developed COVID-19 and 16 did not. The two groups did not differ significantly in key demographics. No volunteers required hospitalization or supplemental oxygen during the study. Every volunteer completed all five follow-up visits. 15 volunteers acquired a non-COVID upper respiratory tract infection in their community between the end of quarantine and the fifth visit at day 360.
The researchers found that the infected group had significantly lower average “baseline-corrected global composite cognitive score” (bcGCCS) than the uninfected group at all follow-up intervals. At baseline, the two groups did not differ significantly. The difference between the two groups did not significantly vary by time, meaning that the infected group’s bcGCCS did not improve during the nearly year-long study.
Because the bcGCCS was a composite based on individual scores for the 11 cognitive tasks, the researchers also looked at which tasks in particular were impacted. They found that the most affected task was related to immediate object memory, in particular, recall of the spatial orientation of the object. There was no difference in picking the correct object itself, just its spatial orientation. This means that infected individuals had a hard time choosing the correct spatial orientation of the object they had just seen, for example, erroneously picking a mirror image of the object they had just seen.
The results were not different based on sex, learning vs. non-learning tasks, or whether individuals received remdesivir or had community-acquired upper respiratory infections.
Because the investigators controlled for so many factors including the strain of SARS-CoV-2, timing of infection, quarantine, and lack of prior infection and vaccination, the study provides high confidence that SARS-CoV-2 infection was responsible for the cognitive defects. The control of the timing of infection also enabled clarification of whether and when cognitive deficits occurred and improved. The differences between the groups were apparent by day 14 of quarantine and as noted previously, the deficits in the infected group did not improve let alone resolve.
The symptom surveys did not differ between the two groups. None of the volunteers, infected or uninfected, reported subjective cognitive issues or symptoms. Thus the infected volunteers with measurable cognitive deficits at one year post-infection were not aware of these deficits.
The study reaffirms prior research into persistent cognitive deficits and brain damage associated with COVID-19, including other studies which have found deficits among patients without symptomatic long COVID. Building upon this prior research, the latest study indicates that basically every single unvaccinated individual with a history of acute COVID-19 is at risk for persistent, measurable cognitive deficits.
Given that other studies have shown that vaccination reduces one’s risk of long COVID by roughly half, similar measurable cognitive deficits are likely prevalent among vaccinated people who suffer “breakthrough” infection, albeit likely at reduced rates of decline.
The study raises the urgent questions about the level of protection provided by vaccination, whether strains since the original “wild type” SARS-CoV-2 strain have similar effects on cognition, and what is the impact of these cognitive deficits on people’s performance at home, work, and school.
The study also adds to the large body of damning evidence that the ruling class’ “forever COVID” policy is of immense criminal proportions. Enabling a dangerous, mind-damaging virus to circulate among humanity worldwide represents a scale of inhumanity and dereliction of duty that is practically unfathomable. The malignity of this intentional policy is underscored by the current situation where the U.S. alone has had over 1 million new infections per day since August, with levels not projected to drop below 1 million until November.
The working class must deepen the struggle to replace the capitalist system that prioritizes profit over lives with a world socialist society that places human needs first.
Study Link: www.thelancet.com/journals/eclinm/article/PIIS2589-5370%2824%2900421-8/fulltext
By Bill Shaw
A new study in eClinicalMedicine has found that healthy volunteers infected with SARS-CoV-2 had measurably worse cognitive function for up to a year after infection when compared to uninfected controls. Significantly, infected controls did not report any symptoms related to these cognitive deficits, indicating that they were unaware of them. The net effect is that potentially billions of people worldwide with a history of COVID-19, but no symptoms of long COVID, could have persistent cognitive issues without knowing it.
The study’s lead author, Adam Hampshire, professor of cognitive and computational neuroscience at King's College London, said:
"It … is the first study to apply detailed and sensitive assessments of cognitive performance from pre to post infection under controlled conditions. In this respect, the study provides unique insights into the changes that occurred in cognitive and memory function amongst those who had mild COVID-19 illness early in the pandemic."
This news comes as pandemic mitigation measures have all but been abandoned by governments across the globe. Public health practice has been decimated to the point where even surveillance data on SARS-CoV-2 infections and resulting hospitalizations, deaths, and other outcomes are barely collected let alone published.
The data that are available indicate, per the most recent modeling from the Pandemic Mitigation Collaborative (PMC) on September 23, that since the beginning of August there have been over 1 million infections per day in the US alone. This level of transmission is expected to persist through the remainder of September and all of October. For the months of August through October, these levels of transmission are the highest of the entire pandemic
The study on cognitive deficits has been shared widely across social media, with scientists and anti-COVID advocates drawing out its dire implications.
Australian researcher and head of the Burnet Institute, Dr. Brendan Crabb, who has previously advocated for a global elimination strategy to stop the pandemic, wrote:
"Ethical issues aside, this is a powerful addition to an already strong dataset on Covid-driven brain damage affecting cognition & memory. Given new (re)infections remain common, this work… should influence a re-think on current prevention/treatment approaches."
The study enrolled 36 healthy volunteers. These individuals had no history of prior SARS-CoV-2 infection, no risk factors for severe COVID-19, and no history of SARS-CoV-2 vaccination. The researchers determined whether the volunteers were seronegative prior to inoculation, meaning that they had no detectable antibodies to SARS-CoV-2. If such antibodies were present, it would indicate past infection or vaccination.
These procedures resulted in a total of data from 34 volunteers being included for analysis. Two volunteers were excluded from analysis because they had seroconverted to positive for SARS-CoV-2 antibodies between the time of screening and inoculation. Notably, these two volunteers participated in all subsequent study activities, enabling a sensitivity analysis of the results that included them.
The researchers inoculated all 36 volunteers with SARS-CoV-2 virus in the nose and then quarantined them for at least 14 days. Volunteers only returned home once they had two consecutive daily nasal and throat swabs that were negative for virus. Thus, those volunteers who had an infection after inoculation spent the duration of their infection in quarantine. This quarantine was required by ethical study protocols, in order that the study itself not increase community transmission of the virus.
The researchers collected data on the volunteers daily during quarantine and at follow-up visits at 30, 90, 180, 270, and 360 days post-inoculation. The assessments included body temperature, viral loads from throat and nasal swabs, surveys on symptoms, and computer-based cognitive tests on 11 major cognitive tasks. The cognitive testing varied the particular exercise for each of the 11 tasks to avoid learning and memorization of solutions in subsequent sessions. Nevertheless, some tasks were more prone to learning so the researchers also studied the effect of infection on “learning” vs. “non-learning” tasks.
Of the 36 inoculated volunteers, 18 became infected and developed COVID-19 and 16 did not. The two groups did not differ significantly in key demographics. No volunteers required hospitalization or supplemental oxygen during the study. Every volunteer completed all five follow-up visits. 15 volunteers acquired a non-COVID upper respiratory tract infection in their community between the end of quarantine and the fifth visit at day 360.
The researchers found that the infected group had significantly lower average “baseline-corrected global composite cognitive score” (bcGCCS) than the uninfected group at all follow-up intervals. At baseline, the two groups did not differ significantly. The difference between the two groups did not significantly vary by time, meaning that the infected group’s bcGCCS did not improve during the nearly year-long study.
Because the bcGCCS was a composite based on individual scores for the 11 cognitive tasks, the researchers also looked at which tasks in particular were impacted. They found that the most affected task was related to immediate object memory, in particular, recall of the spatial orientation of the object. There was no difference in picking the correct object itself, just its spatial orientation. This means that infected individuals had a hard time choosing the correct spatial orientation of the object they had just seen, for example, erroneously picking a mirror image of the object they had just seen.
The results were not different based on sex, learning vs. non-learning tasks, or whether individuals received remdesivir or had community-acquired upper respiratory infections.
Because the investigators controlled for so many factors including the strain of SARS-CoV-2, timing of infection, quarantine, and lack of prior infection and vaccination, the study provides high confidence that SARS-CoV-2 infection was responsible for the cognitive defects. The control of the timing of infection also enabled clarification of whether and when cognitive deficits occurred and improved. The differences between the groups were apparent by day 14 of quarantine and as noted previously, the deficits in the infected group did not improve let alone resolve.
The symptom surveys did not differ between the two groups. None of the volunteers, infected or uninfected, reported subjective cognitive issues or symptoms. Thus the infected volunteers with measurable cognitive deficits at one year post-infection were not aware of these deficits.
The study reaffirms prior research into persistent cognitive deficits and brain damage associated with COVID-19, including other studies which have found deficits among patients without symptomatic long COVID. Building upon this prior research, the latest study indicates that basically every single unvaccinated individual with a history of acute COVID-19 is at risk for persistent, measurable cognitive deficits.
Given that other studies have shown that vaccination reduces one’s risk of long COVID by roughly half, similar measurable cognitive deficits are likely prevalent among vaccinated people who suffer “breakthrough” infection, albeit likely at reduced rates of decline.
The study raises the urgent questions about the level of protection provided by vaccination, whether strains since the original “wild type” SARS-CoV-2 strain have similar effects on cognition, and what is the impact of these cognitive deficits on people’s performance at home, work, and school.
The study also adds to the large body of damning evidence that the ruling class’ “forever COVID” policy is of immense criminal proportions. Enabling a dangerous, mind-damaging virus to circulate among humanity worldwide represents a scale of inhumanity and dereliction of duty that is practically unfathomable. The malignity of this intentional policy is underscored by the current situation where the U.S. alone has had over 1 million new infections per day since August, with levels not projected to drop below 1 million until November.
The working class must deepen the struggle to replace the capitalist system that prioritizes profit over lives with a world socialist society that places human needs first.
Study Link: www.thelancet.com/journals/eclinm/article/PIIS2589-5370%2824%2900421-8/fulltext